
Key Takeaways
1. Medicare telehealth coverage disappeared for 43 days in late 2025 after Congress missed a renewal deadline.
2. More than 4 million Medicare beneficiaries relied on telehealth before the shutdown.
3. Families faced cancelled appointments, delayed care, out-of-pocket costs, and avoidable health setbacks.
4. Congress restored coverage, but the underlying problem remains: telehealth access is still tied to temporary extensions.
5. The next major deadline is December 31, 2027 — and families should prepare now. Three simple planning steps can help protect your family's care plan before the next deadline.
When Care Pauses, Disease Doesn't
Martha Swick used the phrase “taking a step back.”
Her husband Bill, 53, has corticobasal degeneration; a rare brain disease that has taken his ability to feed himself, dress himself, and travel to Chicago for the speech therapy appointments that were slowing its progression. For the past several years, those appointments happened by video. Then, on October 1, 2025, they stopped. Not because Bill’s condition changed. Because Congress missed a deadline.
For 43 days, Bill and Martha practiced old strategies instead of learning new ones. The disease kept moving. The care plan didn’t.
That is what a Medicare telehealth shutdown looks like from inside a living room. Not a policy disruption. Not a coverage lapse. A family practicing old strategies while a disease moves forward, because a benefit they built their care plan around was never, in any legal sense, permanent.
What the shutdown actually was, and how 4.3 million people found out the hard way
Most families who use Medicare telehealth don’t think about where it comes from. It’s there. It works. The doctor appears on the screen. That sense of normalcy is exactly what made October 1, 2025 so disorienting.
On that date, the telehealth flexibilities that had kept virtual care available to Medicare beneficiaries since the pandemic simply expired. Congress hadn’t cut them. Hadn’t changed them. Had simply failed to renew them before the deadline, and in the absence of a renewal, the default kicked in: no coverage.
The scale of who this affected was not small. According to research from Brown University’s Center for Advancing Health Policy through Research, 4.3 million Medicare beneficiaries used telehealth in the first half of 2025 alone — primarily to manage behavioral health conditions, diabetes, hypertension, and chronic kidney disease. STAT News reported that in 2024, 6.7 million traditional Medicare enrollees; 25% of those eligible, used a telehealth service. These were not casual users. These were people managing serious, ongoing conditions through regular virtual appointments.
For families like Susan Collins’, telehealth was never optional. Her late husband Leo had progressive supranuclear palsy — a rare brain disorder — and getting him to his doctors required a 60-mile round trip that became increasingly impossible as his condition progressed. Telehealth, she said, was “a tremendous relief,” according to the Associated Press. October 1 removed that relief without notice, without transition, and without explanation to the families who depended on it.
The numbers tell you how many people were affected. The living rooms tell you what it actually meant.

A cancelled virtual appointment highlights the impact of lost telehealth access.
What it actually meant — cancelled appointments, ER visits, and a two-month wait
The statistics tell you the scale. The individual accounts tell you what the scale was made of.
Vicki Stearn, 68, from Bethesda, Maryland tried to schedule a virtual visit with her doctor during the shutdown. She was told Medicare had ceased telehealth coverage. The earliest in-person appointment available was December; a wait of more than two months. She opted to pay out-of-pocket for the telehealth session, hoping for reimbursement once the government reopened, according to NPR. She was one of the fortunate ones. She could pay.
For patients managing chronic conditions, the gap was not just inconvenient. It was clinical. Dr. Faraz Ghoddusi, a family medicine provider in Tigard, Oregon, told the Associated Press that he uses telehealth to monitor patients with diabetes and chronic lung disease. During the shutdown, one of those patients missed their regular check-ins, and ended up in the emergency room.
Across health systems, the response was systematic. Hospitals posted notices that read: “Due to the federal government shutdown, Medicare and Medicaid patients are unable to schedule new telehealth/video visits,” ABC News reported. This was not a case-by-case disruption. It was a structural one — the same notice, the same cancellation, the same wall, across providers nationwide.
Congress eventually provided retroactive reimbursement for claims filed during the lapse. What it could not reimburse was Vicki Stearn’s two-month wait, or the emergency room visit that might have been a routine check-in, or the regression Martha Swick watched her husband experience while the calendar moved and therapy did not. Retroactive coverage makes the books balance. It does not make the care happen. [For families who want to understand what Medicare telehealth currently covers — and how to verify what their parent’s plan includes, read the Medicare Telehealth Coverage in 2026].
Why is this Important?
The 43-day shutdown revealed a problem many families never knew existed: the telehealth services they rely on are not guaranteed. For millions of Medicare beneficiaries, virtual care is no longer a convenience, it is part of how they manage ongoing treatment. When that access disappears, even temporarily, care does not simply pause. Conditions continue to progress.
The pattern behind the crisis; why this keeps happening and what would have to change
The 43-day shutdown was not the first time families came close to losing Medicare telehealth coverage. It was the latest time.
Since the pandemic-era flexibilities were first introduced in 2020, Congress has extended them repeatedly, never by making them permanent law, always by attaching them to short-term budget resolutions that required renewal before the next deadline. Each extension bought time. None of them bought certainty. The American Medical Association said it plainly in May 2025; four months before the shutdown proved them right: “A permanent fix is needed.”
What happened in the fall of 2025 was not a surprise to anyone watching the legislative calendar. The flexibilities were set to expire September 30. Congress did not act. They lapsed. Forty-three days later, a resolution extended them, but only through January 30, 2026, according to the American Occupational Therapy Association. That meant families had roughly ten weeks before the question opened again. Congress acted a second time in February 2026, extending coverage through December 31, 2027, as Senator Brian Schatz’s office confirmed.
Two resolutions in four months. A benefit that millions of families depend on, renewed twice in a single winter, each time under deadline pressure.
Bipartisan bills to make the flexibilities permanent have been introduced — the CONNECT for Health Act among them, endorsed by AARP — but none have passed. The American Hospital Association has endorsed permanent legislation. The AMA has endorsed it. The votes to pass it have not materialized. Until they do, the December 31, 2027 extension is not a resolution. It is the next deadline.
Understanding that pattern is the first step. The second is knowing what to do before it arrives.

Missed check-ins show how quickly chronic care can be disrupted.
What to do before 2028
The families who fared worst during the 43-day shutdown were not the ones who had bad luck. They were the ones who had no plan B. Vicki Stearn had to choose between paying out-of-pocket and waiting two months. Bill Swick had no alternative. Dr. Ghoddusi’s patient ended up in the ER. None of those outcomes were inevitable. All of them were the result of a care plan that treated a temporary benefit as a permanent one.
The next deadline is December 31, 2027. Here is what to do before it arrives.
- Know which parts of your parent’s care plan depend on telehealth. List them specifically — which appointments, which providers, which conditions are being managed virtually. Then identify which of those providers offer in-person alternatives and how long it would take to get one scheduled. Do this now, not in November 2027.
- Establish behavioral health telehealth from home before December 31, 2027. Mental health and behavioral health telehealth is the one category that survives permanently — no location requirement, no facility rule, ever. If your parent starts those visits from home before the deadline, they qualify as an established patient and can continue with only one in-person visit per year. That window is open now. It will not stay open indefinitely.
- Build the shutdown question into your next care conversation. Ask your parent’s providers directly: if telehealth coverage lapses again, what is the contingency? A provider who has thought about this is a provider worth keeping.
The extension through 2027 is real. The relief it offers is real. And the vulnerability that produced two winters of near-misses is also real — and has not been resolved. [Our full guide to what telehealth covers in 2026 and what changes in 2028] is the place to understand the current landscape. This article is the place to understand how fragile it has been — and what that means for the plan you build around it.
Non Medical Disclaimer
The information provided in this article is for educational purposes only and is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read in this article.
Related Posts

Remote Patient Monitoring: The Home Care Technology That’s Quietly Changing Everything
There's a particular kind of math you do without meaning to. The last time you talked to your parent. Whether anything in their voice was off. Whether the two days since then mean nothing, or mean…

Medicare Telehealth Coverage in 2026: What Seniors Can Use From Home Right Now
Two things are probably true right now. The first: you've heard that Medicare telehealth got complicated — something about a shutdown, something about rules changing — and you're not entirely sure…
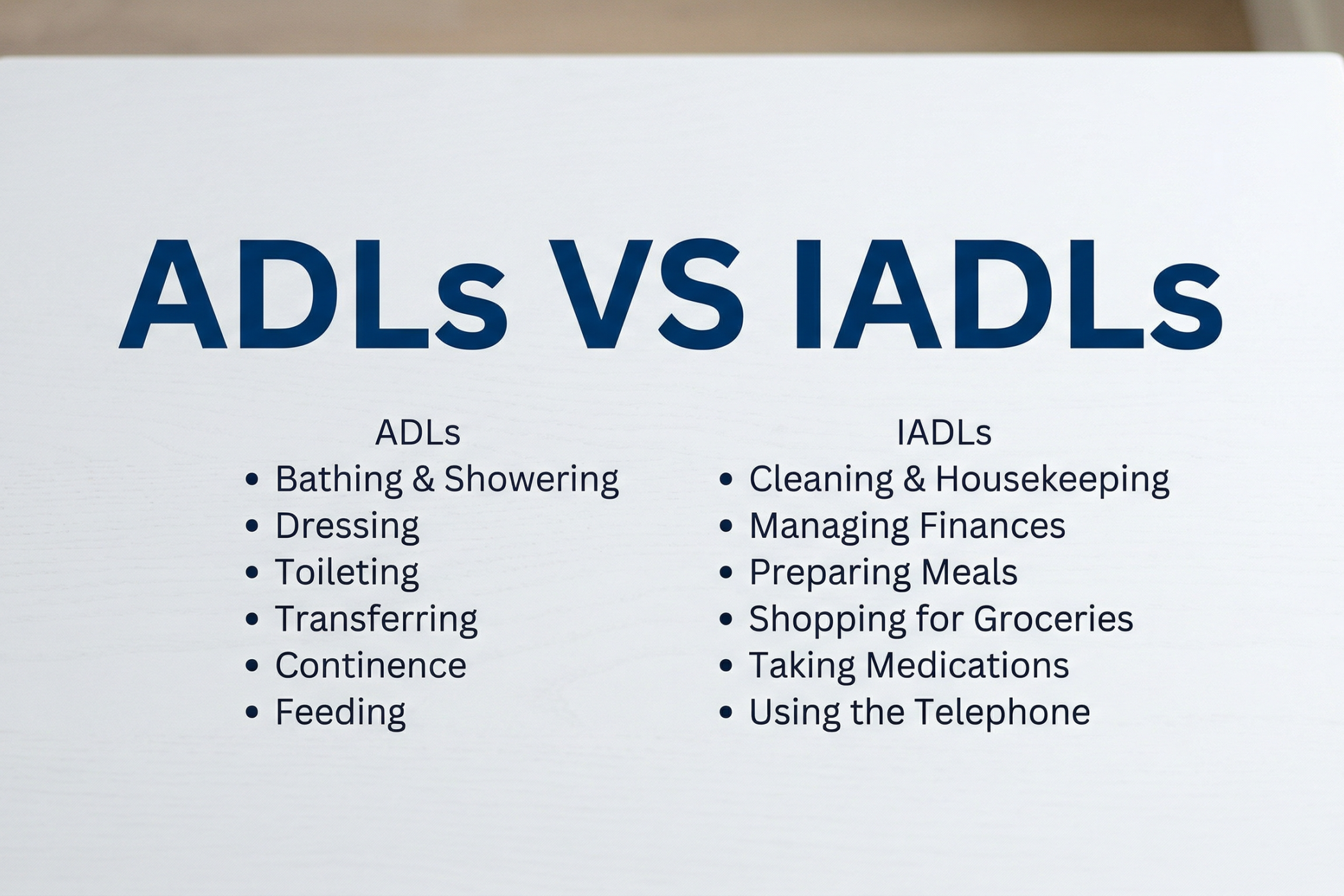
ADLs vs IADLs in Brain Injury: A Non-Medical Guide for Families
When a loved one returns home after a brain injury, the biggest challenges are often the ones you can’t see. You might notice they can walk to the kitchen or get dressed without help, yet they still…
